

As physician compensation transitions from a fee-for-service model into some form of pay for performance, therapeutic strategies are increasingly focused on targeting the root causes of disease. In January this trend took the form of the Endocrine Society’s releasing new clinical-practice guidelines calling for a paradigm shift in treating obesity and its comorbidities: Rather than waiting for problems like high blood sugar, hypertension and elevated cholesterol to develop, the guidelines advise practitioners to target obesity itself, thus avoiding or reducing future complications.
When diet and exercise fail, newly approved medications for weight management should be prescribed, the study suggests. Therapies for diabetes, depression and other chronic diseases should be chosen with an eye toward promoting weight loss. “Knowledgeable prescribing of medications, choosing whenever possible those with favorable weight profiles, can aid in the prevention and management of obesity and thus improve health,” the authors conclude.
Since 2012, four new obesity drugs have gained FDA approval. Sales of Belviq and Qsymia have been lackluster so far, but the industry has high hopes for the two newest arrivals, green-lit in the last six months: Contrave and Saxenda. The sales push will be ambitious. Orexigen will enlist help from Japanese pharmaceutical giant Takeda’s 900-strong US sales force in marketing Contrave, a combination of popular antidepressant Wellbutrin and the anti–substance abuse agent naltrexone. To promote Saxenda, a differently dosed version of Novo Nordisk’s diabetes blockbuster Victoza, the company has announced plans to dedicate 500 US reps to the job.
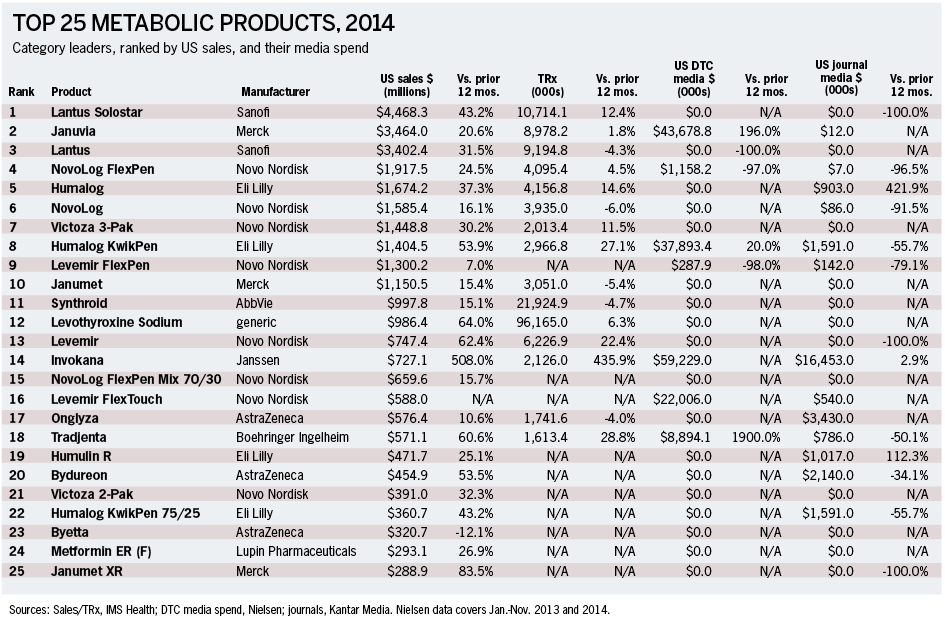
CLICK HERE to see the Top 25 Metabolic Products for 2014
It’s going to be an uphill battle. The 1990s Fen-Phen recall looms large in the collective medical mind, plus the weight loss achieved by new obesity drugs continues to be modest, in the 5% to 10% range. And insurers have been reluctant to cover weight-loss therapies.
On the other hand, it is probably a battle worth fighting. With 80 million Americans now obese and two out of every three adults overweight or obese, the epidemic offers huge potential for co-morbidity reduction and healthcare cost savings. Studies show that even modest weight reduction can result in significant overall health benefits. Also, if doctors and patients take to these therapies, carriers will be forced to cover them eventually. Indeed, a significant improvement in the obesity epidemic should reduce overall costs for health insurers.
Moreover, given the growing overlap be-tween diabetes care and weight-loss strategies, pharmaceutical companies see a strong position in the metabolic market. For example, there has been a surge of interest in glucagon-like peptide (GLP-1) agonists—the class to which Saxenda belongs—mainly because of their appetite-suppressing qualities. Conversely, makers of Qsymia are seeking FDA approval to treat diabetes.
Contrave and Saxenda have not undergone head-to-head trials. Opinions on efficacy vary but by and large their ability to reduce weight appears even. Contrave has the double advantage of coming in pill form (in contrast to the injection-delivered Saxenda) and of being priced lower than its rival.
However, among general practitioners and specialists who treat diabetes, Saxenda is similarly esteemed as Victoza—which controls 70% of the GLP-1 agonist market, generated $2 billion for Novo last year and boasts a long-term safety record. “Previously we’ve always been worried about what to give a person who has borderline diabetes but wants to lose weight,” says Rachel Pessah-Pollack, MD, FACE, clinical assistant professor at the Icahn School of Medicine at Mount Sinai, department of endocrinology, diabetes and metabolism. “Now we have a good option to treat them. Not a lot of long-term data exists on some of the oral meds. To have a medication we’re familiar with is really a good option.”
It is also unclear how much negative impact Saxenda’s delivery system will actually have. Obese patients will go to great lengths to lose weight, according to John Foreyt, PhD, director of the Behavioral Medicine Research Center at Baylor College of Medicine and one of Contrave’s investigators. “Obviously, taking a pill is easier, but if a drug is really effective, people have no problem injecting,” he says, and studies prove as much. Avoiding an invasive and risky bariatric surgical procedure is also a strong motivator, he adds.
Non-insulin options
For the past several years, diabetes care has functioned in the shadow of the ACCORD study. In 2008, ACCORD (Action to Control Cardiovascular Risk in Diabetes) was one of three trials aimed at assessing different levels of therapy intensity on cardiovascular health. Researchers abruptly halted the study when a 22% increase in mortality emerged among patients undergoing intense glycemic-control therapy, mostly caused by cardiac events.
This finding sent shock waves through the diabetes world that continue to reverberate today. No one knows for sure what caused the surge in deaths, but hypoglycemia has been the primary suspect. Pre-ACCORD diabetes strategy mostly involved hammering away at HbA1c, without much thought to hypoglycemia. Post-ACCORD strategies focus on individualized treatments, easing back on glycemic targets when hypoglycemic risk arises. Since insulin is known to cause hypoglycemia and weight gain, a deluge of non-insulin drugs has come to market in recent years.
The hottest class among such drugs is GLP-1 agonists, a k a incretin mimetics—gastrointestinal hormones that generate insulin after meals and slow digestion. The dominant GLP-1 agonist is Victoza, facing competition from Eli Lilly’s new entry, Trulicity, approved last year. Both appear evenly matched at lowering blood sugar but Trulicity’s once-a-week dosing schedule trumps Victoza’s once-a-day. But studies show Victoza induces slightly more weight loss.
GlaxoSmithKline’s Tanzeum also gained approval last year but in clinical trials failed to prove non-inferiority to Victoza, so Novo sees it as less of a threat. Tanzeum offers a once-a-week schedule.
AstraZeneca’s two forms of exenatide, the short-acting Byetta and the long-acting Bydureon, have been around for several years. Valued for its once-a-week dosing schedule, Bydureon has nonetheless been panned as difficult to use. In response, the manufacturer debuted a new injection pen last year—which has spurred an uptick in sales, according to the company.
Last year concern arose about a study suggesting a link between pancreatitis and GLP-1 agonists. But after scrutinizing the paper, European regulators and the FDA issued statements questioning its findings’ validity, concluding there was little evidence of increased pancreatitis, which in any case is a known complication of diabetes.
Sanofi’s Lyxumia, a once-daily GLP-1 agonist, has been available in Europe since 2013 and the company hopes to submit the drug for FDA approval sometime this year. Sanofi also has a Lyxumia-glargine combo drug in Phase-III trials called LixiLan. Although Novo’s patent on Victoza does not expire until 2020, the company is already developing Victoza’s potential replacement, semaglutide, which is in Phase-III trials. Evidence suggests semaglutide might be longer acting and promote better cardiovascular outcomes.
The most significant side effect associated with GLP-1 agonists is nausea. “Some patients just can’t tolerate the upset stomach,” says Sinai’s Pessah-Pollack. “But part of the reason these drugs are so popular with clinicians is that a bit of stomach upset and nausea helps with the weight loss. So it’s a fine line we have to walk.”
Otherwise the most notable downside of GLP-1 agonists is their method of delivery: injection. Many diabetes patients loathe needles. A deplorable reality of diabetes care is that a large population of patients who should be taking insulin is not solely due to needle fear.
Enter the pill-delivered sodium-glucose cotransporter 2 (SGLT-2) inhibitors, the newest class of non-insulin agents. These drugs work by lowering the reabsorption of blood sugar by the kidneys. Patients lose some sugar by urinating. By bypassing the insulin process completely, these drugs avoid hypoglycemia.
Of the three SGLT-2 inhibitors approved by the FDA since 2013, Invokana (Johnson & Johnson), Farxiga (AstraZeneca) and Jardiance (Boehringer), none have undergone head-to-head studies. At this point the only notable distinction among them is that patients on Farxiga need to display stronger kidney function. Although new, this drug class is gaining traction. Invokana grossed about $300 million in the first three quarters of 2014, for example. There are at least five other SGL-2 inhibitors in the pipeline, including ertugliflozin, being developed in collaboration with Merck and Pfizer, and luseogliflozin, which gained approval in Japan last year.
One curious SGLT-2 inhibitor attribute is that there appears to be a ceiling on their glucose-inhibiting ability. Urinary glucose excretion does not increase even at the highest doses. “There are a couple of studies that suggest perhaps the liver is kicking up glucose production, as the body’s way of compensating,” says Edward Chao, DO, associate clinical professor of medicine at the University of California, San Diego School of Medicine. “But that is still a hypothesis.” Inducing dual SGLT-2 and SGLT-1 inhibition or combining an SGLT-2 inhibitor with a GLP-1 agonist or a dipeptidyl peptidase-4 (DPP-4) inhibitor might overcome this limitation, he adds.
With so many options available and imminent, education efforts will likely play an important role, according to Marc Sirockman, EVP/GM of agency Artcraft Health, which lists Novo Nordisk on its roster. Current patient-outreach strategies favor a positive-reinforcement approach.
“We’re going to see more educational programs that have an underlying element of fun to them,” Sirockman predicts, adding that patient choice will move to the forefront. “In oncology, hemophilia, HIV and a lot of other fields, patients have a give-and-take conversation with their healthcare provider about their therapy. Diabetes hasn’t gotten there yet, but it will eventually.”
CLINICAL CORNER
As patent cliffs go, Sanofi could have far worse chances for a soft landing after its blockbuster Lantus patent expires this year. For one thing, potential generic rivals face long delays before entering the US market, giving the Paris-based drugmaker time to promote what it hopes will be Lantus’s successor, Toujeo. Meanwhile, last month the company launched the world’s only inhalable insulin product.
 Although approved in Europe, Eli Lilly and Boehringer Ingelheim’s biosimilar Lantus generic is still subject to a court-ordered 30-month stay in the US, the result of Sanofi’s patent suit. And Novo Nordisk’s Tresiba, which is said to control hypoglycemia even better than Lantus, will be excluded from the US until 2017 or later while the company conducts FDA-mandated studies on potential cardiovascular risks.
Although approved in Europe, Eli Lilly and Boehringer Ingelheim’s biosimilar Lantus generic is still subject to a court-ordered 30-month stay in the US, the result of Sanofi’s patent suit. And Novo Nordisk’s Tresiba, which is said to control hypoglycemia even better than Lantus, will be excluded from the US until 2017 or later while the company conducts FDA-mandated studies on potential cardiovascular risks.
Toujeo, a concentrated version of Lantus, offers different pharmacokinetics, making it more effective, Sanofi says. In studies, the new drug sparked a particularly low rate of hypoglycemia in the initial eight weeks of therapy. Early-phase treatment is especially important because that’s when titration occurs. In addition, the intensified concentration of the drug prolongs its duration of effect, thus reducing the risk of nighttime hypoglycemia, the company adds.
Sanofi hopes to convince the five million patients currently taking Lantus or Novo Nordisk’s Levemir to switch to its new basal insulin, which is expected to gain FDA approval in the first quarter of 2015. It will also target newly diagnosed patients, potentially expanding its market by a million patients a year.
Launched in February, Sanofi’s inhalable Afrezza is the only option for patients who require mealtime insulin but want to avoid an injection or who want to start insulin but cannot face the needle. It will compete against Eli Lilly’s Humalog and Novo’s Novolog.
The insulin market has long been ripe for a non-injection option. Several companies have experimented with inhalers but none has achieved success. In 2007 Pfizer withdrew its inhaled product, Exubera, due to lack of patient acceptance. Complaints focused on the device’s being too large, clumsy and inconvenient.
Sanofi’s device, by all accounts, is small and easy to use. However, user convenience is not what the diabetes world is concerned about. A year after being withdrawn, Exubera was linked to increased risk of lung cancer, causing worries Afrezza might pose a similar risk.
“I have some reservations about the potential toxicities of insulin inhalants,” says Zachary Bloomgarden, MD, FACE, clinical professor of medicine at the Icahn School of Medicine at Mount Sinai, department of endocrinology, diabetes and metabolism. Both coughing and reduced lung function were observed in Afrezza subjects, he notes. He also points out that insulin is a growth-promoting hormone, which could encourage the proliferation of cancer cells.
“We feel we are in a good position here [in terms of safety],” responds Stefan Schwarz, the Afrezza US lead, regarding the potential safety concerns. “The drug has been approved by the FDA and deemed safe and efficacious for use by patients.” He added that Sanofi will continue to monitor patient safety as the product is introduced.
From the March 01, 2015 Issue of MM+M - Medical Marketing and Media







{kind=link}